This may be a long one...
")
As you might have expected I voted option 2. I do not want for one second to be cured of my autism, but I do wish to see society cured of it's ignorance. Co-occurring conditions are not autism and can be treated separately.
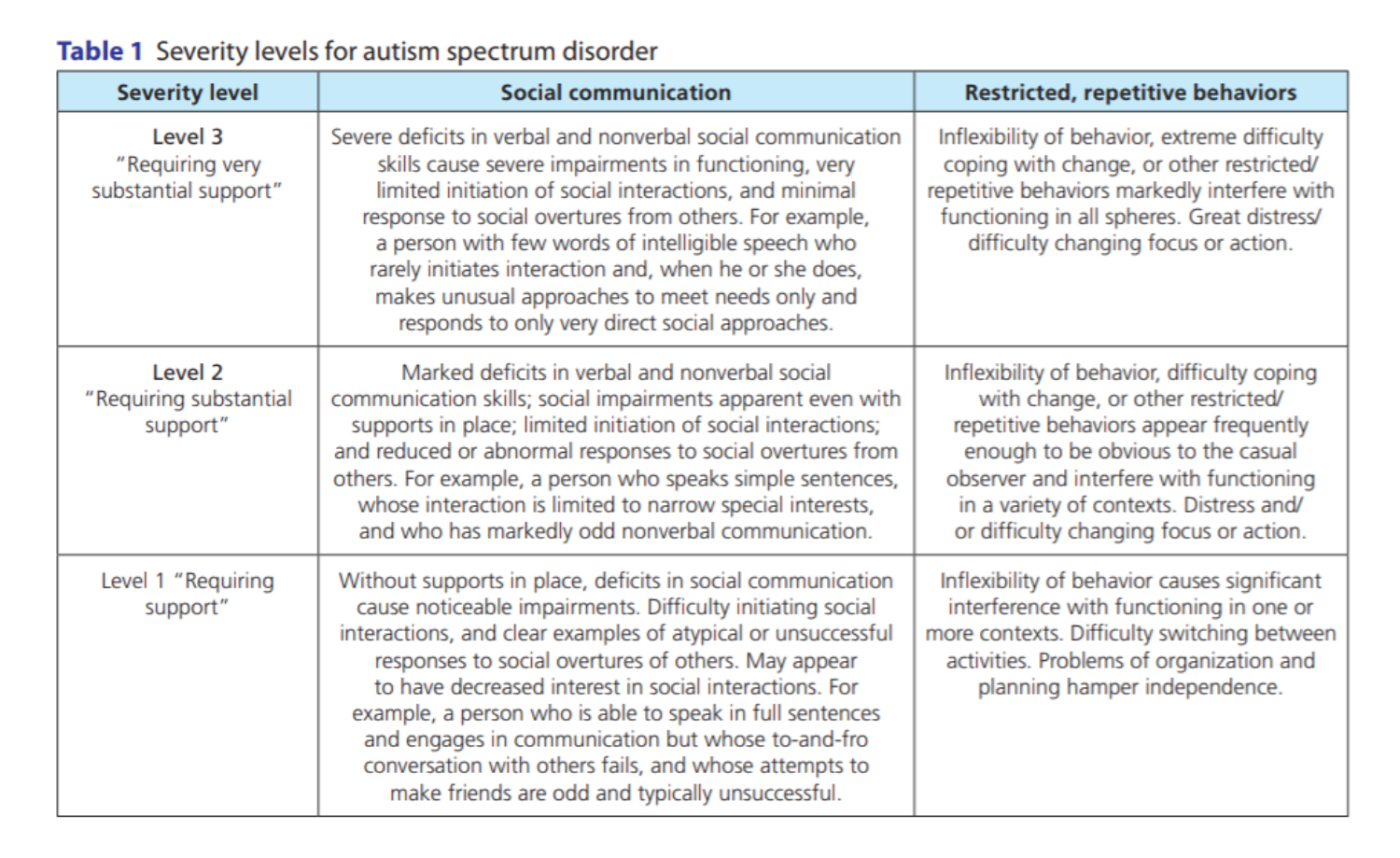
To clarify the classifications of ASD 1/2/3.
All designations include co-occurring conditions which may be physical or mental conditions. Anxiety and depression are remarkably common amongst ASD1. Less common but still frequent are ADHD, Dyspraxia, Dyslexia, OCD, various GI problems and more. The presence of at least 1 co-occurring condition is expected and looked for in the current diagnostic process.
The current ASD subdivisions are based on care/support needs.
The thing we must keep in mind about co-occurring conditions is although their presence is considered a facet of ASD by science, they are all conditions which are also experienced by NT people.
Our different brain wiring, including our hyper/hypo-sensitivities is autism. Depression, anxiety, GI problems, IDDs, ADHD etc. are not. They are parallel to our being autistic and in some cases we have a higher likelihood of having these side conditions pro-rata, than non autistic people.
Cures or treatments for these conditions will benefit far more NT people than Autistics and in many cases treatments exist. My anxiety and depression has been treated with SSRIs and (attempts at) therapy. My GI problems have been treated with various drugs to control my acid levels and with anti-emetics. BPD and ADHD have established drug treatments that work for a great many people and so on... None of these is prevention or or cure, but they do make the lives of millions of people more comfortable.
There is a separate debate about whether or not drug companies have the incentive to truly seek cures due to the rolling profits generated by symptomatic control, which I don't want us to go into here, but the fact remains that these conditions are often treatable. If they only affected autistic people the numbers would be so low that the treatments wouldn't exist, or the prices would be astronomically high (fancy a £500 bottle of Gaviscon anyone?)
Unfortunately there is no known cure for IDDs (or Learning Disabilities as they used to be called) and the causes of those are manifold. Foetal alcohol syndrome has already been mentioned, and a huge proportion of IDDs can be traced to lifestyle and environment. Epigenetic changes can alter the male gamete before conception. Pollution, alcohol, smoking, diet, obesity and many other factors can affect the foetus in utero. Short of gene scans of sperm prior to fertilisation and complete genetic scans of the early stage foetus, it will be very difficult to practically prevent many IDDs with environmental causes. Amnioscentesis can be used to detect broad chromosomal information such as Downs and gender, but more precise information such as identifying autism or many IDDs is a very long way off.
Consequently, any attempt to prevent autism by selective termination would be a scattergun approach, akin to breaking eggs with a sledgehammer. Many more viable foetuses would be aborted than necessary since there is such an element of doubt. It must also be remembered that the relevant genes so far identified only point to the
potential of autism, not a guaranteed autistic birth. There have been occasional cases of identical twins with exactly the same genome, one of whom has been autistic and the other not. There are also uncertainties because the same gene expressions so far found in autism occur frequently within the general population. The present theory suggests that autism is the result of a large number of genetic expressions which, in certain combinations, may lead to the person being autistic.
When we consider what autism is at it's core - an uneven distribution of sensory and cognitive abilities, the question of a cure becomes even more unpalatable for some. I have mentioned before that we, as autistic people, present "spikey profiles" when we are assessed. Our strengths are matched by our weaknesses, whereas NT people have much more even distributions, as shown in the simplified diagram below.

The theory goes along the lines of each individual being born with a number of individual "skillpoints" (as some RPG players will be familiar with). The typical NT profile is that of a generalist, with the points relatively evenly distributed between dozens of different skill traits. Autistic people have Spikey profiles because their skillpoints are distributed unevenly. Very high in some areas and equally low in others. Most commonly social skills are quite low, but logic, reason, linguistic or artistic skill could be much higher than the average. The extreme case is the savant, who may be quite low across the board but spike extremely highly in a narrow area.
This where the "cure for autism" hits it's biggest problem. If you find a cure or preventative measure, those peaks will drop as the troughs are raised. If you "cure" poor social skills, something else has to give. To answer the question from
@55853 above, if you cure our autism, you also cure the attributes so many of us hold dear. Speaking for myself, I may gain social confidence, improve my Theory of Mind and lose my auditory sensitivities, but I would lose my linguistic skill, my sharp hearing and my creativity to pay for it. It is not a price I am
willing to pay since it essentially would make me into a different person.
Another thing to consider with the most common co-occurring conditions of anxiety and depression. It has been posited that both conditions are an inevitable
result of the pressures we face living in a society that we often have limited understanding of. Many of us face discrimination, hostility and marginalisation. The majority of us are out of work and short of money. Our living conditions may be poor as a result. Those are conditions which would lead anybody, including NTs into such unwanted mental states. It has been observed that autistic people living in better conditions with understanding and accepting people around them suffer less anxiety and depression than those who don't. It stands to reason then, that improved outcomes for integration and employment lead to less co-occurring mental health problems.


 )
)