Thank you for this information Tiffany Kate.That infographic is a very simplified one. It's sometimes useful to give people simplified information because it's easier to understand the basics - but sometimes, things get simplified too far.
Another thing to remember is what audience the simplified information is aimed at, because things might be deliberately missed out or simplified because the author thinks it's something that isn't important for their target audience to know.
With that infographic, it seems to me that the target audience isn't autistic people aiming to understand their diagnosis, or professionals trying to diagnose autism - it's more aimed at the general population who might find themselves dealing with an autistic person. So it's aimed at describing what autism might look like from the outside. For instance, I'm level 1, and that description is pretty accurate for how I present in general day-to-day life. However, if you get to know me, you'll find that I definitely have "high interest in specific topics", it's just that I don't talk about them unless it comes up. Likewise, I do have some repetitive behaviours, but not such that it's noticeable day-to-day unless you're paying close attention.
The diagnostic criteria for autism are the same regardless of whether it's level 1, 2, or 3 (Clinical Testing and Diagnosis for Autism Spectrum Disorder) - what makes it Level 1, 2 or 3 is the severity of the symptoms.
When you go through the diagnostic procedure for autism, they're not just looking at how you present day-to-day, doing your best to "act neurotypical". They're actively aiming to find the "real you", underneath any tricks and techniques you may have learned to disguise or deal with your autistic-ness. This gets more important the older you are, as you may be "masking" without knowing it in some ways, because you have learned to do/not do certain things by trial and error and now they are just part of how you present to the world.
So during a diagnostic interview, they won't just be listening to what they say, they'll be evaluating how you say things and actively watching what you do.
Diagnosis is a lot more complex than this. It's also important to remember that:
- Autism and ADHD are spectrum disorders, and an individual will often have more significant problems with some areas than others.
- For many people (especially adults), they will have learned ways to cope with any deficits they have which results in those deficits not being as noticeable (which is the whole point!). As an outside observer, you may not be able to spot or know about the training/practice/techniques the person uses to disguise or work around their deficits.
Writing a long post on a forum is a good example of how you only see the end product, not the process that went into it. There may have been a lot of re-drafting and pulling-back of wandering attention in the process... but all you see is a tidy post and not all the blood, sweat and tears that went into it.
For example, in day-to-day life, I have a reputation for being exceptionally well-organised. ("Forget? You? You never forget anything," said someone recently). What they don't see is the amount of time and trouble I take to seem that way. I know that if I don't put every single thing on my to-do list immediately then it will go out of my head and won't get done. I can't remember more than two instructions of any list (the first two or the last two). So I have to write it down. If a task is not on my list, I won't start it even if I do remember it (sometimes not even then). If I don't have a nice visual representation of all the projects I'm dealing with, I can't remember them and something will slip through the cracks. My appearance of being well-organised is actually an over-correction of a certain amount of executive dysfunction. But that's not what people see.
I was conerned a bit when I read about the Level 3 areas as some people live alone and have to be responsible for themselves and I didn't wish more than I what I was measured at. Some time out it is what I thought and try and forget and move on.
I think this the second time I seen a mention of rocking etc in Level 3 diagnosing. Perhasps they both use the same source.
Moving on
I have read some conversation in this thread about eye contact.
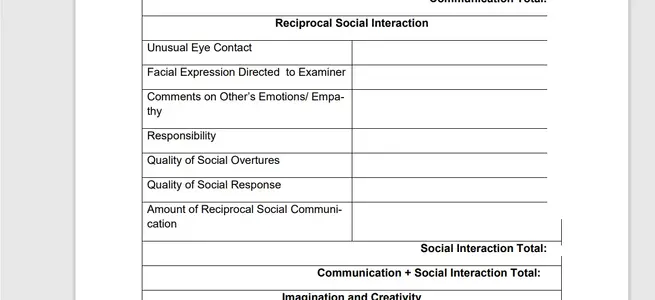
Now the ADOS reads quite strange don't look at the examiner too much or then you score highly in at least 1 lol.